

Firearms Police officers undergo an extensive training programme in line with the national firearms curriculum; this includes the medical module referred to as D13. This sets out the national medical course for firearms officers; it was introduced, with guidance from the FPHC, in 2010.
D13 provides comprehensive first-aid training, aiming to equip frontline officers with the capability to deal with the initial management of commonly encountered medical emergencies. First audited in 2016 (FL Hartley, 2017), this re-audit looks at Patient Report Forms (PRFs) from two large metropolitan police forces in the subsequent twelve months to examine whether the course meets the demands of the role.
2017 saw the highest number of offences involving a knife or sharp instrument since 2011, a 22% increase on the previous year. It also saw an 11% increase in firearm offences (National Office for Statistics, 2018). Since 2010, eight terror related attacks have taken place, five since the last audit. The police are often the first on scene, and the demand is on officers to provide urgent lifesaving treatment in highly challenging environments. This alone highlights the importance of adequate medical training.
152 PRFs were analysed, the majority of incidents (59%) were not firearms call-outs. The officers were faced with a wide range of incidents (Figure 1) with varying degrees of severity. Some extremely challenging incidents were dealt with and examples of excellent care predominate. In particular three terror incidents and multiple casualty calls were attended; exceptional examples of triage and decision making, with prompt effective care in high pressure environments, were illustrated.
Key Findings
The majority of PRF’s begin with space to record patient demographics and details surrounding the date, time and location of the incident. The form then goes on to establish mechanism of injury, injuries found and treatments/interventions utilised. This is often broken down into the A to E assessment format used by the officers. On many of the forms there is also space for free text, allowing the officers to record a brief history of events. Data was gathered and analysed from all aspects of the forms. The varying degree of quality of form filling is likely to be having a significant impact on our findings. However the key findings of the audit, in several specific areas of interest, are summarised below.
1. Chest exposure and examination
51% of assault victims had their chest exposed, and 15 chest injuries were identified. For those victims involved in stabbing or shootings 45.5% of chests were exposed and 11 injuries identified. For those involved in vehicle collisions; 52% were exposed with 5 injuries found. Importantly, these figures do not take into account the range of factors that may influence the decision to expose patients; however these groups are at relatively high risk of having an unidentified chest injury. Gender of the patient had some influence, with 43% of female assault victims exposed compared to 51% of male victims.
2. Oxygen Use
The D13 manual states that all trauma patients should receive high flow oxygen. 40% of all patients and 35% of assault victims received oxygen, a lower figure than found in the previous audit (51%). After discounting those who refused oxygen, oxygen was given to 70% of those with identified breathing difficulties, 47% of chest injuries and 71% of CAT bleeds. These numbers should arguably be higher, although this does not take into account factors such as quick ambulance arrival, lack of resources or multiple patients.
3. C-spine Injuries
There were 68 cases identified in which consideration of C-Spine injuries would be indicated. However, in only 22 of these cases were such injuries suspected by the officer, with only 9 receiving MILS. A range of reasons including: patient refusal, on-going CPR or collar use by ambulance crews, prevented MILS from being carried out.
4. Pelvic Injuries
In 50% of cases where MOI was suggestive of pelvic injury and use of pelvic binder may have been appropriate, there was no evidence of a pelvic binder having been considered or used. As previously stated, this does not take into account all influencing circumstances, but may be an area for future review.
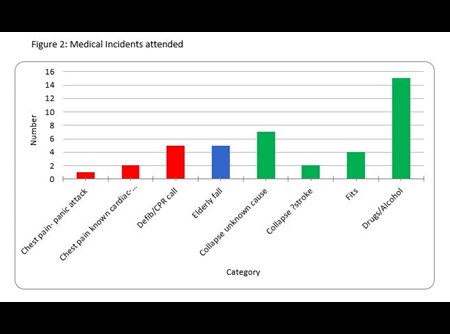
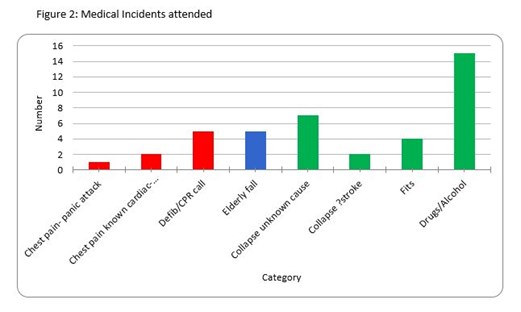
5. Medical cases
Medical cases are defined as and include elderly falls of less than 6 feet, defib/CPR calls, collapse of any cause and where drugs +/- alcohol have been causal either through loss of consciousness or minor falls (Figure 2). The focus of the D13 course is often teaching on injuries caused by assaults. While this forms the single biggest category, this audit highlights the broad range of incidents officers will need to be equipped to deal with. No training course could cover everything, and with limited time and resources, training courses must continue to strive to provide officers with a simple approach to dealing with medical incidents. This audit has highlighted the crucial role well trained officers have played in saving lives, and illustrated areas for continued improvement. The motto “Simple things done well, always” should be reinforced.
 6. Time on Scene
6. Time on Scene
An average of 48 minutes was spent on scene, however not enough information is available to analyse how much time of this time was actually spent dealing with casualties. Furthermore there are numerous reports of delays awaiting ambulance transport, and there was at least one recorded incident where a patient was transported in a police car due to lack of ambulance availability.
There are many examples where excellent care was found to be given. This was particularly highlighted in the case of a young teen; both effective lifesaving care and admirable clinical judgement were applied. The patient had received a single stab wound to thigh and was likely peri-arrest at time of officers’ arrival due to massive blood loss. Family members had attempted to unsuccessfully stem the bleeding and a tourniquet was correctly applied by the officers stopping further blood loss. Crucially, key signs of deterioration were spotted leading to a rapid transfer to hospital in the police vehicle. The patient received immediate surgery and after four days in hospital had made a full recovery.
Currently each police force is using a different PRF form. Although they largely capture the same data, the variations make direct comparisons challenging and a missed opportunity to gather key information. A new generic PRF is in development, this aims to ensure all forces gather data uniformly, and will allow forces to learn from one another through easier compilation of a national database. This will ultimately be used to further improve training, allowing officers experiences to directly inform the curriculum.
This re-audit further stresses the importance of medical training received by firearms officers; and is illustrating the huge impact they have on saving lives with simple, timely and effective techniques. In conjunction with developing a new PRF this audit and future audits will focus on shaping appropriate and effective training to enable firearms officers to continue to save lives.
Report written by:
Dr Fiona Hartley MBChB
Dr Philippa Serebriakoff MBBS BSc
Select a year and month from the headings below to view news items from that month.
Due to essential systems maintenance and upgrades there will be intermittent interruptions to some on-line services on Saturday 27th of February. There will be further interruption to some core services on Wednesday 2nd and Thursday 3rd of March.
We apologise for any inconvenience caused.
× Back to News Home
Back to News Home